
The Merit-based Incentive Payment System is CMS’s new attempt to control Medicare Spending. This program consolidates three existing programs and one new program, in order to derive a MIPS score, from 0 to 100, which can significantly impact a provider’s Medicare reimbursements for each payment year.
Starting in 2017 (the first performance year), MIPS will annually measure performance of Medicare Part B providers; incentive payments or negative penalty adjustments will begin in 2019 (the first payment year). MIPS combines three existing programs: the Physician Quality Reporting System (PQRS), the Electronic Health Record (EHR) Meaningful Use Program, and the Value-Based Modifier (VBM) program, and one new program called Clinical Practice Improvement.
As of now, the three existing programs offer rewards or penalties to Medicare Part B providers based on quality measures and providers' ability to demonstrate certain capabilities. In 2017, they'll be consolidated and all go under the MIPS umbrella.
For the first two years of MIPS CMS has deemed physicians, physician assistants, nurse practitioners, clinical nurse specialists, and nurse anesthetists Medicare Part B providers as eligible professionals. As you can see the list of eligible professionals starts out with the highest level providers but quickly expands to cover a large majority of providers.
More EPs will be added in 2019. These EPs include physical or occupational therapists, speech-language pathologists, audiologists, nurse midwives, clinical social workers, clinical psychologists, and dietitians or nutrition professionals will be deemed as eligible professionals for the Merit Based Incentive Payment System.
Furthermore, a provider group including such eligible professionals for each respective year will also be deemed eligible as a group entity for MIPS by means to be defined in the MIPS final rule. Some components of MIPS, such as PQRS, already support the concept of group measurement. However, other components, such as MU, only measure individual providers. Therefore, the MIPS final rule will need to define how individual MU performance is rolled up to determine group MIPS performance.

So how does MIPS plan to succeed in controlling spending by Medicare on physician services, where other pieces of legislation have failed? It plans to utilize three existing programs (Meaningful Use, the Physician Quality Reporting System, and the Value-Based Modifier (VM) Program) and one new program (called Clinical Practice Improvement).
In short, MIPS consolidates and strengthens the financial impacts of these programs, while continuing their performance measurement and reporting mechanisms that have become familiar to providers over the last few years.
By combining existing incentive programs, MIPS will create a composite performance score, of 0-100, that will influence a healthcare provider's reimbursement rates. The four performance categories that will be measured are:
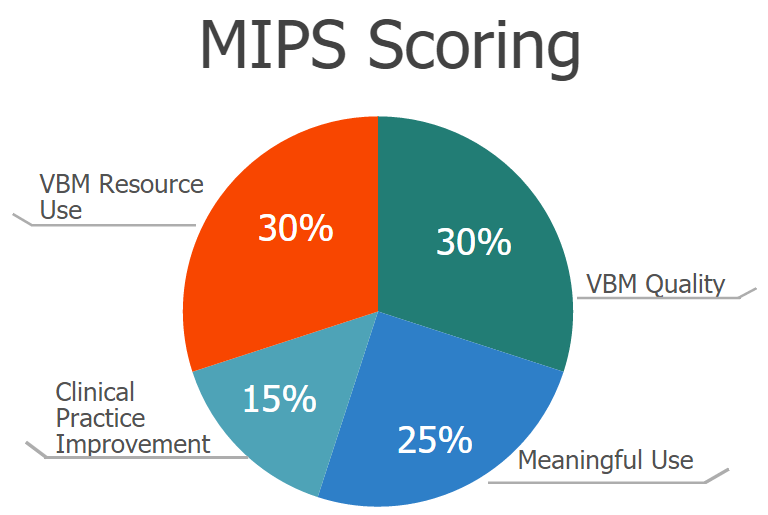

The Centers for Medicare and Medicaid Studies (CMS) has requested recommendations from stakeholders to identify practice improvements in these categories (to which more categories may be added later):
There are varied payment methodologies being developed by payers for health care services. Payers are moving away from fee-for-service (FFS) volume-driven health care services to value-based payment models that incentivize providers on quality, outcomes, and cost containment.
In the near future it is likely that your practice will feel the impact as payment models move away from FFS to other payment formulas. The intent is to promote patient value and efficiency, but one consequence is to shift some risk to you, the physician provider. Practice viability will be dependent on how well quality, cost, and efficiency are managed.
Accountable Care Organizations (ACOs), patient Centered Medical Homes, and bundled payment models are some examples of APMs.
The first payment year is set to be 2019, and because MIPS follows the same 2-year lag of similar programs, 2017 is set to be the first performance year of MIPS. For the 2017 performance year (and the respective 2018 payment year), three programs (MU, VBM, and PQRS) will continue as separate and distinct measurement and payment adjustments until the 2017 performance year, at which time they will be consolidated with the fourth and new program (clinical practice improvement) to generate a provider’s MIPS score.

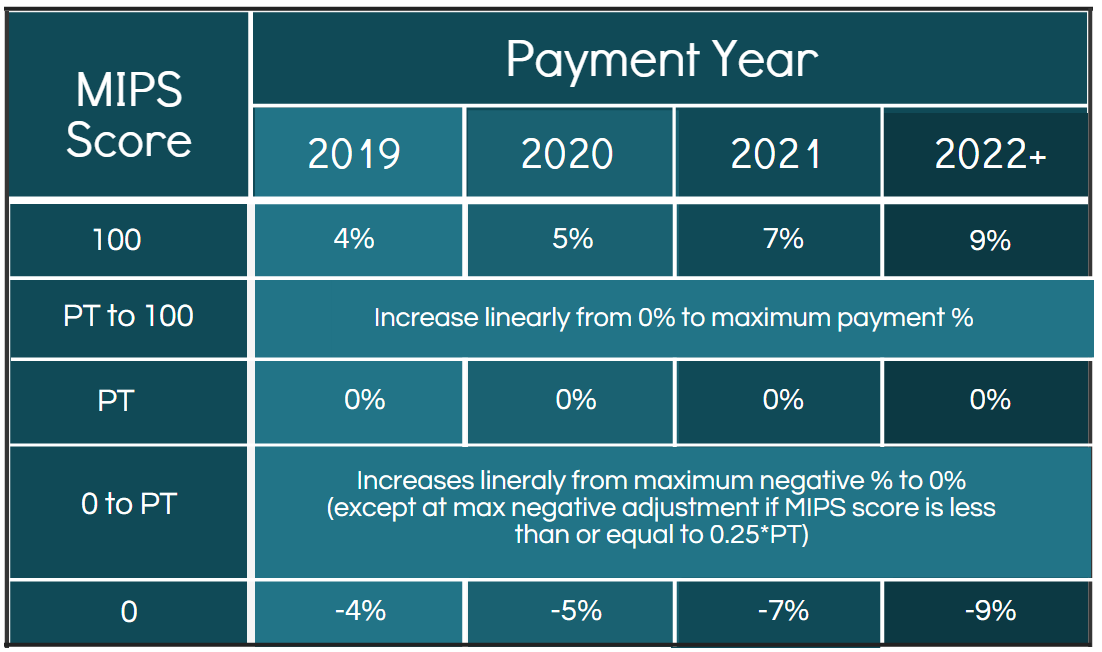
The performance threshold (PT) is the demarcation MIPS score between positive or negative adjustments and is determined every year as the mean or median of the MIPS scores for all EPs in a prior period as selected by CMS. The PT will likely be specified in an annual CMS final rule which will be published prior to each performance year.
The scores in between the maximum positive and negative adjustments are calculated on a linear basis. For example, if the PT is set at 40 and provider A scores a 35 while provider B scores a 20, provider A’s negative reimbursement would be just below 0% (around -0.5%), while provider B’s negative reimbursement would be lower than that (around -2.0%). The only exception is at the max negative adjustment if the MIPS score is less than or equal to 0.25 * PT. For example, if the PT was set at 40, then a score of (40*0.25) 10 or below would garner the max negative adjustment.